






Healthcare data security standards define what organizations must protect, but they do not identify every affected cloud resource, service account, encryption key, backup, identity provider, or business associate integration.
In 2024, the US Department of Health and Human Services received 663 reports of breaches affecting 500 or more individuals. Those reports covered approximately 242.9 million affected individuals. HHS notes that the figures are approximate, and the same person may be represented in more than one breach report.
This article focuses on US healthcare data security requirements and the engineering work required to operate them across AWS, Microsoft Azure, Google Cloud, Kubernetes, SaaS, VMware, and hybrid infrastructure.
Regulatory status: HHS still presents the HIPAA Security Rule modernization published on January 6, 2025, as a proposed rule. The proposed requirements discussed below are not current mandatory HIPAA obligations. This content is for educational purposes and is not legal advice.
TL;DR
- Map requirements to live infrastructure. A policy or framework mapping is incomplete until it identifies the affected assets, expected technical state, accountable owner, evidence source, and failure response.
- Prioritize with healthcare context. Scanner severity alone does not reflect the risk to ePHI or clinical operations. Add exposure, privilege, service criticality, recovery dependency, exploitability, and compensating controls.
- Treat evidence as historical. A current export cannot prove that MFA, encryption, logging, or backup controls operated throughout an audit period. Preserve configuration history, exceptions, remediation records, and retest results.
- Reassess controls when cloud scope changes. New accounts, privileged identities, vendor integrations, ePHI data flows, public exposure, and failed recovery tests should trigger a new risk analysis and control evaluation.
- For cloud security architects: Use the standards map to define which AWS, Azure, GCP, Kubernetes, SaaS, and hybrid resources enter the ePHI control boundary.
- For compliance engineers and CISOs/GRC: Connect healthcare data security regulations to current asset scope, control ownership, exception decisions, and audit evidence.
- For DevSecOps and platform owners: Convert access controls, encryption, audit controls, vulnerability management, and recovery requirements into executable checks and validated closure.
- To compare available solutions, see our review of the 16 best healthcare data security software tools.
What are healthcare data security standards?
Healthcare data security standards are laws, regulations, implementation guidance, control models, and assurance mechanisms used to protect health information from unauthorized access, modification, loss, and disruption.
For cloud security engineers, these sources serve different purposes. Some establish legal obligations. Others help translate those obligations into technical controls or provide assurance that selected controls operated within a defined scope.
| Source | Primary role |
|---|---|
| HIPAA Security Rule | Establishes administrative, physical, and technical safeguards for electronic protected health information |
| HITECH Act | Expands breach-notification, enforcement, and business associate obligations |
| NIST SP 800-66 Rev. 2 | Connects HIPAA Security Rule requirements with practical security activities and NIST controls |
| NIST CSF 2.0 | Organizes cybersecurity outcomes across Govern, Identify, Protect, Detect, Respond, and Recover |
| HITRUST CSF | Provides a structured healthcare control and assurance model |
| ISO/IEC 27001 | Defines requirements for an information security management system |
| SOC 2 | Assesses controls for a defined service and review period |
| GDPR | Establishes legal requirements for relevant personal and health-data processing |
A healthcare organization may use several of these sources at the same time. HIPAA can define the legal requirement, NIST can support implementation, and HITRUST, ISO 27001, or SOC 2 can support assessment or third-party assurance.
But they are not interchangeable. A HITRUST certification or SOC 2 report covers a defined assessment scope. It does not automatically prove that every AWS account, Azure subscription, GCP project, Kubernetes cluster, SaaS application, or business associate environment handling ePHI is correctly configured.
The engineering task is to map each applicable requirement to the relevant cloud assets, technical control, owner, and evidence source. Those implementation mechanics are covered in the sections below.
For a broader comparison, see Cloud Security Compliance Standards. For the evidence and control lifecycle, see Cloud Security Compliance.
Why healthcare data security requires more than compliance
Healthcare data security privacy and compliance programs overlap, but they address different operating risks. Privacy governs permitted use and disclosure, while security controls must preserve the confidentiality, integrity, and availability of the systems processing that data.
IBM’s 2025 Cost of a Data Breach Report estimated the average healthcare breach cost at $7.42 million and an average lifecycle of 279 days to identify and contain an incident. These figures describe the study population rather than the expected impact for every organization, but they show how long investigation, recovery, and operational disruption can continue.
The technical consequence depends on which part of the environment fails.
| Security objective | Example failure | Healthcare impact |
|---|---|---|
| Confidentiality | Unauthorized access to patient or insurance data | Privacy harm, fraud exposure, breach investigation, and notification |
| Integrity | Modification of clinical records, prescriptions, device settings, or identity data | Clinicians and operational teams can no longer trust the affected information |
| Availability | Loss of access to EHRs, communications, identity services, or connected medical systems | Care delivery, diagnostics, scheduling, billing, or recovery may be delayed |
Healthcare technology leader Charles Aunger describes cybersecurity as a patient-safety issue because attacks can disrupt access to patient histories, prescriptions, communications, and medical-device functions. His operating model extends beyond the data store itself: A known vulnerability on an isolated device with restricted network access and active monitoring presents a different risk from the same vulnerability on a device using default credentials, communicating over an unsegmented network, and supporting a critical clinical workflow.
A known vulnerability on an isolated device with restricted network access and active monitoring presents a different risk from the same vulnerability on a device using default credentials, communicating over an unsegmented network, and supporting a critical clinical workflow.
For a cloud security engineer, this changes remediation priority. CVSS or scanner severity is only one input. The decision also needs:
- ePHI scope
- Internet and network exposure
- Human and non-human access
- Clinical or operational dependency
- Availability of patches or vendor mitigations
- Compensating controls
- Accountable owner
- Recovery impact
A medium-severity issue on a shared identity, integration, or recovery service may require faster action than a higher-scoring finding on an isolated development resource.
The broader operating risks are covered in Healthcare Data Security Challenges, while recurring incident patterns appear in Healthcare Data Breaches.
US healthcare data security regulations: HIPAA, HITECH, and state laws
Healthcare data security compliance in the USA starts with HIPAA and HITECH, supplemented by applicable state laws, contracts, and requirements determined by the entity, data, jurisdiction, and service relationship.
HIPAA Privacy, Security, and Breach Notification Rules
The HIPAA Security Rule establishes national standards for protecting ePHI through administrative, physical, and technical safeguards. HHS defines its objective as ensuring the confidentiality, integrity, and availability of ePHI created, received, maintained, or transmitted by regulated entities.
The rule is risk-based. It does not prescribe one AWS architecture, one encryption mode, or one logging stack. The regulated entity must:
- Conduct an accurate and thorough risk analysis
- Select controls appropriate to its environment and risk
- Document security decisions
- Evaluate control effectiveness
- Update safeguards as systems and threats change
HIPAA implementation specifications are classified as required or addressable. Addressable does not mean optional. The organization must determine whether the measure is reasonable and appropriate and document the decision and any equivalent alternative.
For a deeper cloud-specific interpretation of HIPAA, see HIPAA Cloud Security guide.
HITECH and business associate accountability
HITECH expanded breach-notification and enforcement provisions and increased direct obligations for business associates.
A business associate agreement defines contractual responsibilities, but the technical implementation still needs to prove:
- Approved services for ePHI
- Covered accounts and tenants
- Administrative access paths
- Available audit logs
- Encryption and key-management responsibility
- Data and backup locations
- Subprocessor participation
- Incident-notification workflow
- Data return and destruction
- Architecture changes affecting scope
Breach notification requirements
HIPAA notifications generally must be provided without unreasonable delay and no later than 60 calendar days after discovery, subject to the applicable recipient and reporting requirements.
That deadline makes evidence quality operationally important. An organization that cannot determine the affected systems, users, records, and event timeline will struggle to assess the breach scope.
Useful evidence includes:
- Authentication and data-access logs
- Cloud control-plane activity
- Administrative changes
- Network events
- Resource and identity relationships
- Data-flow records
- Incident decisions and timestamps
State and international requirements
HIPAA compliance does not automatically satisfy state consumer health-data, privacy, security, or breach-notification requirements.
The compliance applicability map should identify:
- Entities and systems covered by HIPAA
- Data classified as PHI or ePHI
- State laws applicable to the organization and data subjects
- Contractual security requirements
- International requirements for cross-border processing
The applicability map should then connect to resource scope. A legal conclusion stored outside the inventory cannot stop an engineer from deploying a workload into an unapproved service or region.
Proposed HIPAA Security Rule modernization
The January 2025 NPRM proposes more explicit requirements for technology asset inventories, network maps, vulnerability management, access control, documentation, and recovery.
| Proposed requirement | Proposed timing |
|---|---|
| Remediate critical-risk vulnerabilities | Within 15 calendar days |
| Remediate high-risk vulnerabilities | Within 30 calendar days |
| Restore specified critical systems and data | Within 72 hours |
| Business associate notification after contingency-plan activation | Within 24 hours |
| Review specified inventories, analyses, plans, and compliance activities | At least annually |
| Perform vulnerability scanning | At least every six months |
These deadlines remain proposed. They should not be coded into a mandatory HIPAA policy unless a final rule establishes them.
They are still useful architecture signals. An organization cannot meet explicit remediation or recovery deadlines without:
- Current asset inventory
- Severity and exposure context
- Named owners
- Ticket routing
- Exception governance
- Recovery dependency mapping
- Historical evidence
HIPAA Security Rule safeguards mapped to cloud controls
HIPAA safeguard categories become useful to cloud security engineers only when each requirement is translated into a scoped technical condition, an evidence source, and a failure response. The regulation defines the security outcome. Engineering has to determine which resources are covered and how control operation will be tested.
Administrative safeguards: §164.308
Administrative safeguards govern risk analysis, access management, incident procedures, workforce security, and contingency planning. In cloud environments, the main engineering problem is scope.
Risk analysis under §164.308(a)(1)(ii)(A) cannot account for resources that are missing from the inventory or disconnected from their application and owner. A database record without its IAM roles, network paths, encryption keys, backup dependencies, and business service relationships provides an incomplete risk picture.
The minimum dataset should connect:
- A persistent resource identifier and provider hierarchy
- PHI or ePHI classification
- Application, service, and accountable owner
- Internet, private, and third-party exposure
- Current and historical configuration
- Vulnerability and compliance state
- Identity and recovery dependencies
This data changes how findings are handled. A vulnerability on an isolated development instance and the same vulnerability on a shared identity service should not enter the same remediation queue with identical priority.
The safeguard also needs an executable response path. When patching is delayed or impossible, the workflow must define mitigation, segmentation, shutdown, or risk acceptance rather than leaving the issue open indefinitely.
A healthcare CISO participating in a 2026 practitioner AMA described the failure pattern directly: “If you don’t make the tradeoffs explicit and assign ownership, risk just gets absorbed silently into the system.”
Physical safeguards: §164.310
Cloud providers operate physical controls for their own facilities and infrastructure. The healthcare organization still owns the safeguards around endpoints, workstations, removable media, on-premises systems, and administrative access.
Provider assurance reports can support evidence for hosted infrastructure. They do not cover the customer’s laptop fleet, local facilities, biomedical devices, or media-disposal process.
This division becomes harder around connected medical devices. Many devices cannot run the standard endpoint stack, may depend on vendor-controlled firmware, and may be sensitive to active scanning. The control design may therefore rely on passive discovery, segmentation, restricted communication paths, vendor coordination, and compensating monitoring.
The ownership model must include clinical engineering and hospital operations. One healthcare CISO noted that medical-device security efforts fail when security teams proceed without their engagement and support.
Technical safeguards: §164.312
Technical safeguards provide the clearest bridge between HIPAA and cloud configuration.
| HIPAA area | Cloud implementation | Evidence source | Failure condition |
|---|---|---|---|
| Access control, §164.312(a) | IAM roles, MFA, privileged access, emergency access | IAM API, identity platform, access review | Privileged access outside the approved identity path |
| Audit controls, §164.312(b) | Control-plane, identity, data, application, and network logs | Provider logging API, SIEM, log-management platform | Required source disabled, missing, expired, or not reviewed |
| Integrity, §164.312(c) | Versioning, deployment controls, change approval, integrity validation | Configuration history, pipeline record, object history | Unauthorized change or uncontrolled drift |
| Authentication, §164.312(d) | Unique workforce identities, workload identities, credential controls | IdP, IAM, service-account inventory | Shared, dormant, unmanaged, or ownerless identity |
| Transmission security, §164.312(e) | TLS, private endpoints, VPN, network policy, certificate controls | Network configuration, certificate inventory | Unencrypted or unapproved transfer path |
For example, “MFA is required for administrators” should identify privileged roles across all relevant AWS accounts, Azure subscriptions, GCP projects, Kubernetes clusters, SaaS consoles, and backup platforms. The evidence should also show federation state, emergency-access identities, approved exemptions, the last access review, and the responsible reviewer.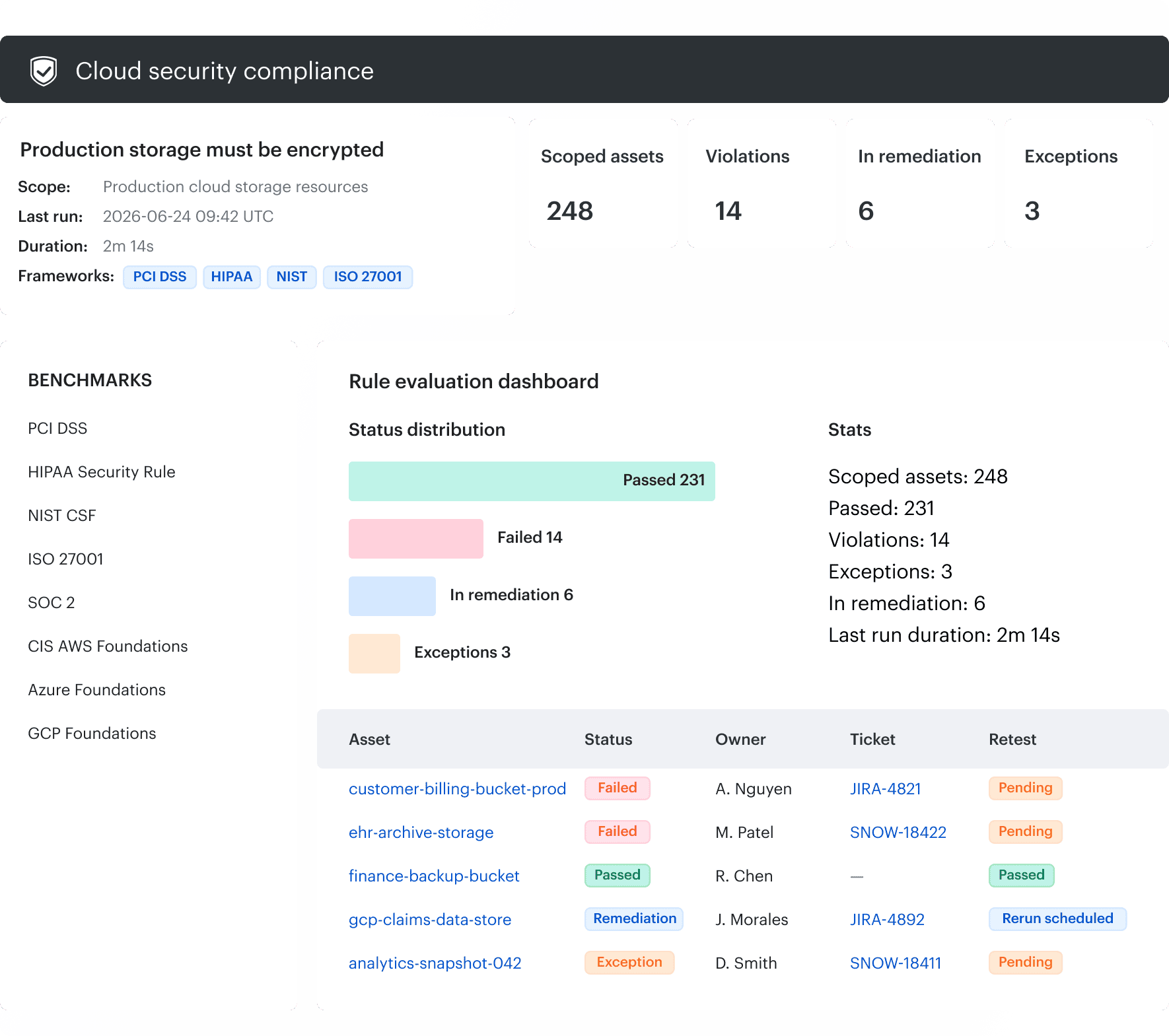 Cloudaware can map one technical policy to multiple standards and track the affected assets through remediation.
Cloudaware can map one technical policy to multiple standards and track the affected assets through remediation.
Logging requires the same level of specificity. A central logging policy does not prove that required sources are enabled in every account or that the security team receives and reviews them. One practitioner in the healthcare AMA observed that some organizations have logging in place but lack monitoring, alerts, and response processing.
That produces a familiar failure chain: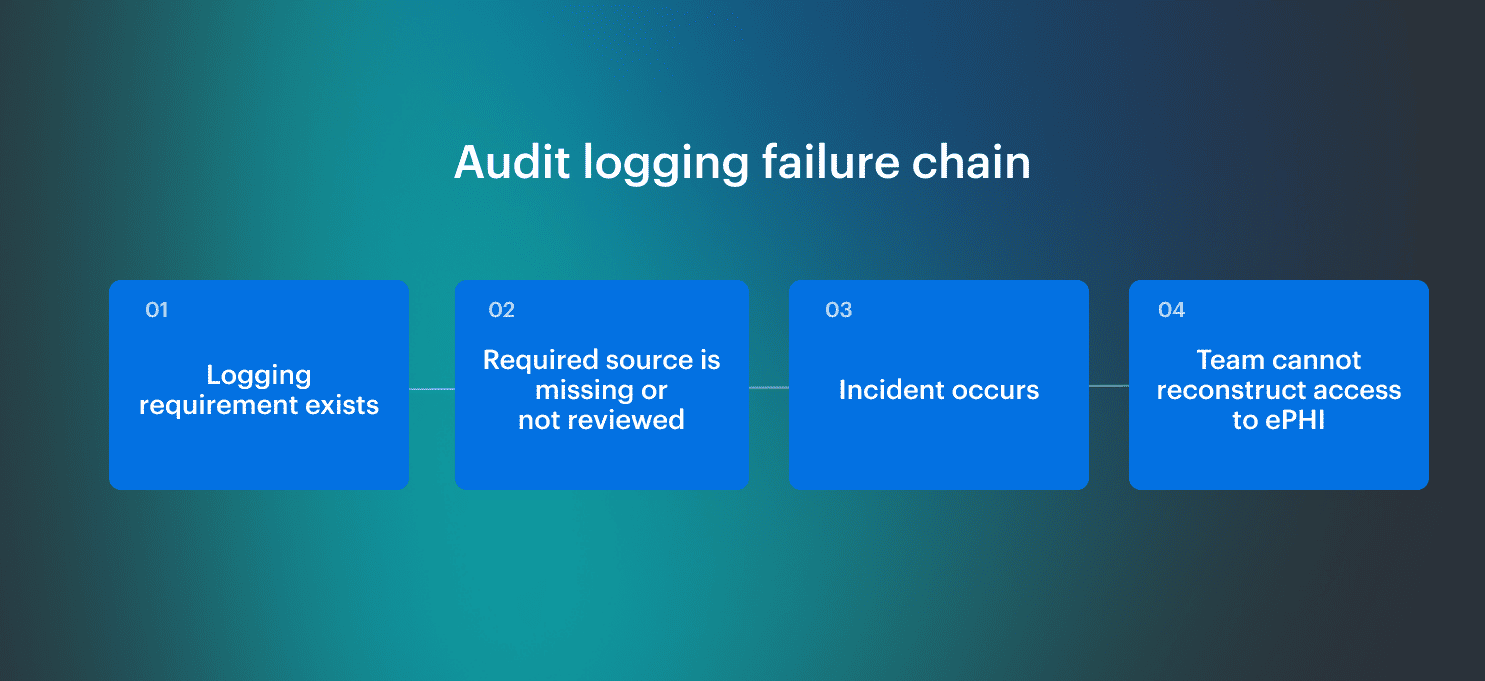 Configuration data proves implementation. Historical configuration, review records, and remediation evidence prove that the control operated over time.
Configuration data proves implementation. Historical configuration, review records, and remediation evidence prove that the control operated over time.
Data security and compliance for healthcare become operational only when each requirement resolves to a defined cloud scope, expected technical state, accountable owner, and evidence source.
Read also: 7 Healthcare Data Security Best Practices for 2026
NIST, HITRUST, ISO 27001, and SOC 2 in healthcare security programs
NIST, HITRUST, ISO 27001, and SOC 2 support different parts of a healthcare security program. None of them removes the need to determine where HIPAA applies or which cloud resources, identities, and data flows fall within scope.
The practical approach is to maintain one internal control model and map it to the requirements, outcomes, and assurance criteria relevant to the organization.
| Source | Main use | Expected output |
|---|---|---|
| NIST SP 800-66 Rev. 2 | Translate HIPAA Security Rule requirements into security activities and control references | HIPAA-to-control mapping |
| NIST CSF 2.0 | Organize cybersecurity outcomes and operating responsibilities | Current-state and target-state security profile |
| NIST SP 800-53 | Select detailed security and privacy controls | Implementable control requirements |
| HITRUST CSF | Define and assess a scoped set of healthcare security requirements | Assessment scope, evidence, and corrective actions |
| ISO/IEC 27001 | Operate an information security management system based on risk | Risk treatment plan, control ownership, and improvement cycle |
| SOC 2 | Evaluate controls operated by a service organization | Assurance report for a defined system and period |
NIST SP 800-66 Rev. 2 translates HIPAA into security work
NIST SP 800-66 Rev. 2 connects HIPAA standards and implementation specifications with practical security activities and NIST control references.
For cloud security engineers, its value is translation: broad requirements such as risk analysis, access control, audit controls, incident response, and contingency planning become work that can be assigned to specific assets, owners, evidence queries, and remediation workflows.
The publication does not identify the organization’s AWS accounts, Azure subscriptions, GCP projects, Kubernetes clusters, or SaaS dependencies, so those mappings still need to be built from the deployed environment.
For a broader NIST implementation view, see NIST Cloud Security.
NIST CSF 2.0 structures the operating model
NIST CSF 2.0 organizes cybersecurity outcomes into Govern, Identify, Protect, Detect, Respond, and Recover. For a healthcare cloud security team, the framework helps check whether the operating model covers risk authority, asset context, technical protection, detection, incident handling, and recovery. It does not prescribe provider-specific settings.
A Protect outcome such as controlled privileged access still needs a concrete implementation for federation, MFA, emergency access, review frequency, evidence, and failure conditions.
HITRUST CSF structures scoped healthcare assurance
HITRUST CSF consolidates requirements and control references into a healthcare-oriented assessment model. Its engineering value comes from defining an assessment boundary and proving that controls operate within it.
Before relying on a HITRUST assessment, teams should verify which services, cloud environments, data flows, customer-operated controls, evidence periods, and corrective actions were included. A provider’s certification does not automatically extend to every customer deployment or configuration.
ISO/IEC 27001 connects cloud controls to risk decisions
ISO/IEC 27001 governs how an organization identifies information security risk, selects treatment, assigns responsibility, evaluates performance, and improves the program.
For cloud security engineers, the useful output is a risk record connected to live infrastructure. A generic entry such as “cloud storage exposure” is difficult to operate unless it resolves to specific storage resources, data classification, provider hierarchy, exposure path, owner, compensating controls, and remediation status.
See ISO 27001 Risk Assessment for the full risk-to-control workflow.
SOC 2 provides assurance, not customer-side configuration proof
SOC 2 evaluates controls for a defined service organization system and review period. Cloud security teams should treat the report as a scoped evidence source rather than proof that the service is secure in every deployment.
The report may confirm provider-side controls while leaving customer responsibilities such as identity lifecycle, administrative access, logging, encryption configuration, and data-path selection outside the assessed scope.
The practical approach is to maintain one internal control model and map it to the requirements, outcomes, and assurance criteria relevant to the organization.
Building a healthcare data security control model
A healthcare data security framework becomes operational through a control model that converts requirements into scoped checks, owners, remediation paths, and evidence.
For every control, engineering needs to know:
- Which assets and data paths are in scope?
- Which state is expected?
- How is failure detected?
- Who owns the response?
- What proves closure?
Build an ePHI dependency graph
The proposed HIPAA Security Rule modernization would require a technology asset inventory and a network map showing how ePHI moves through electronic information systems.
A database-only scope is incomplete. A healthcare workload may also depend on an identity provider, workload identities, encryption keys, APIs, report storage, logging pipelines, backups, recovery accounts, and CI/CD systems.
These dependencies may not store ePHI, but they can expose it, alter the application handling it, or make it unavailable.
The asset model should connect each resource to:
- Provider hierarchy
- ePHI classification
- Application and owner
- Access paths
- Key dependencies
- Integrations
- Backups
- Monitoring coverage
Translate requirements into executable cloud checks
A requirement becomes operational only when it has a technical scope, expected state, failure condition, owner, response, and validation method. For an encryption-at-rest control:
| Control element | Example |
|---|---|
| Scope | ePHI databases, storage, disks, snapshots, and replicas |
| Expected state | Encryption enabled with an approved key configuration |
| Failure condition | Encryption disabled, unapproved key, inaccessible key, or missing evidence |
| Owner | Application, platform, or data-service team |
| Validation | Configuration recheck and recovery test where relevant |
“Encrypted and control-compliant are not identical. A database may be encrypted while an overprivileged principal can decrypt it, a replica uses another key, or the recovery account cannot access the key.” — Igor K., DevOps Engineer at Cloudaware
Define remediation and exception paths
Healthcare systems do not always support the preferred fix. A cloud-native workload may be rebuilt quickly, while a vendor-managed clinical system may require vendor approval or a narrow maintenance window.
An exception needs affected assets, residual risk, compensating control, owner, approver, expiration, and closure condition. It must be reassessed when exposure, architecture, data classification, or resource scope changes.
An exception for one VM should not silently extend to a replica, autoscaling group, second region, or cloned environment.
The operating flow is: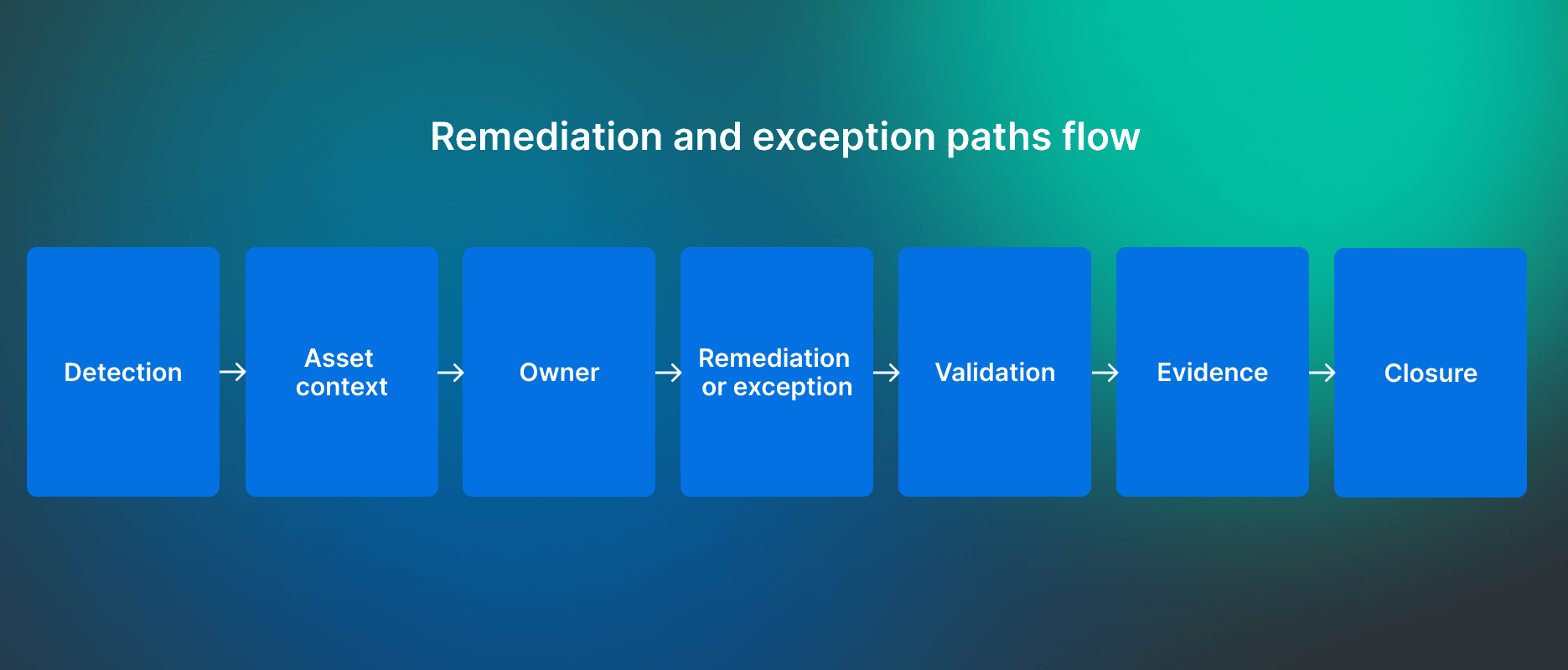 This model also supports cloud security governance by making decision authority and escalation explicit.
This model also supports cloud security governance by making decision authority and escalation explicit.
Essential healthcare data security controls
Healthcare data security controls should be designed around real failure conditions affecting ePHI and clinical operations.
1. Treat identity as the control plane
Healthcare identity includes workforce users, administrators, vendors, emergency accounts, service accounts, API integrations, and workload identities.
A common gap appears when the main application uses SSO and MFA but another path reaches the same data through a local admin account, vendor support identity, embedded credential, or ownerless service account.
The control should cover workforce, privileged, third-party, and non-human access. Evidence should show who or what can access ePHI, through which path, for which application, and under whose approval.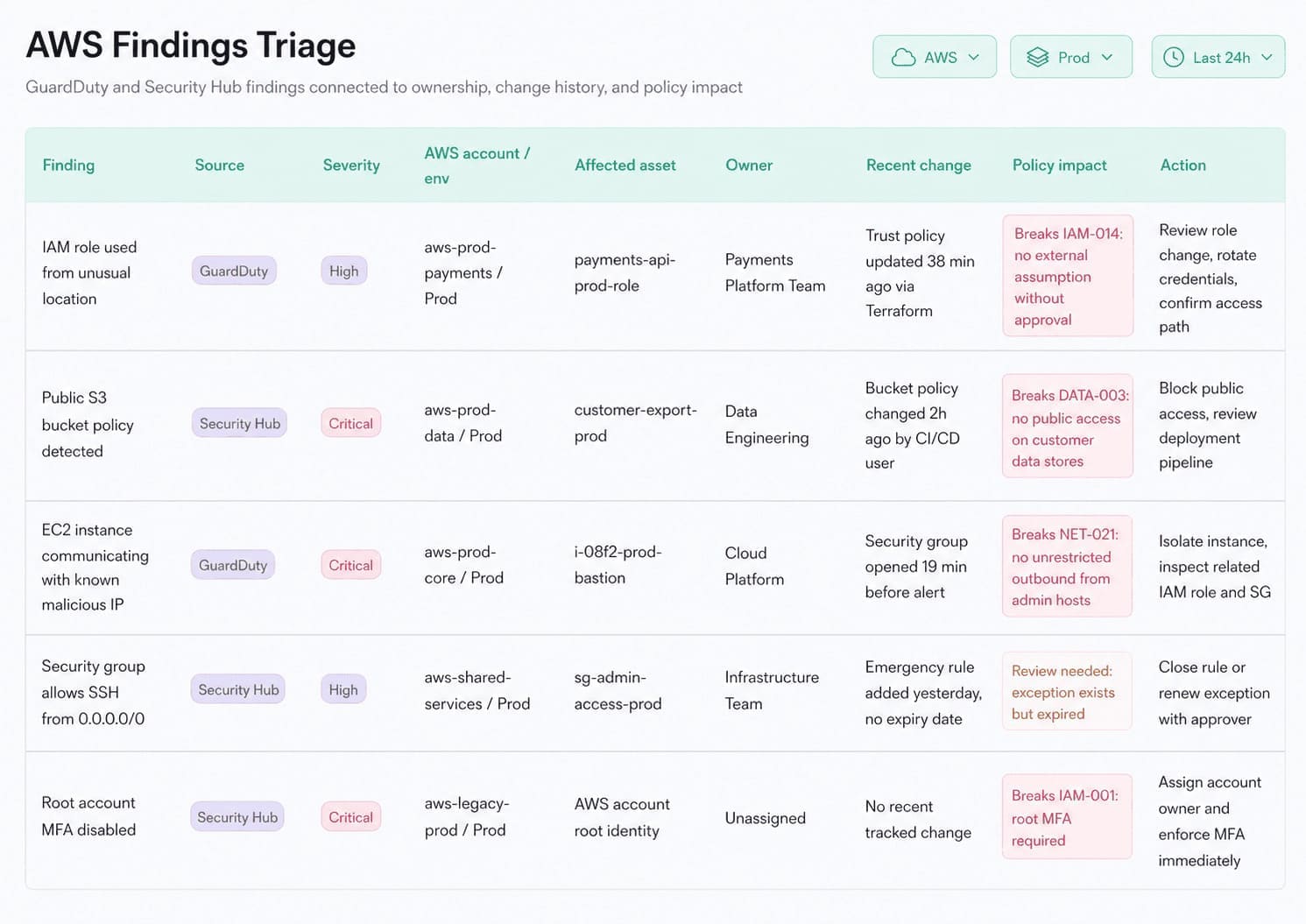 Cloudaware connects a failed access or identity policy with the affected cloud asset and accountable owner.
Cloudaware connects a failed access or identity policy with the affected cloud asset and accountable owner.
2. Validate key dependencies, not only encryption state
HHS’s proposed HIPAA changes would explicitly require encryption of ePHI at rest and in transit, with limited exceptions.
The real control includes the resource, key, key owner, permitted principals, replicas, backups, and recovery environment. Common gaps include overbroad decrypt permissions, unapproved key types, inconsistent replica encryption, unlogged key changes, and key rotation that breaks dependencies.
3. Measure logging by investigation readiness
A SIEM connection does not prove that access to ePHI can be reconstructed. The control should define required identity, control-plane, data-access, application, database, key-use, network, and recovery events for each in-scope service.
Coverage often fails partially:
- Control-plane logs exist, but data-access logs do not.
- A new account is missing from the pipeline.
- Retention is too short.
- Ingestion fails without alerting.
- Alerts are not reviewed.
4. Design vulnerability remediation for healthcare constraints
HHS states that HIPAA risk analysis should include risks from unpatched software. Its proposed modernization also includes vulnerability scanning and penetration-testing requirements.
- A containerized service may be rebuilt and redeployed.
- A vendor-controlled clinical system may require segmentation, restricted communication, passive monitoring, vendor escalation, or retirement.
- Prioritization should combine severity with ePHI scope, exploitation, exposure, privilege, clinical criticality, recovery dependency, finding age, and compensating controls.
This prevents a high scanner score on an isolated test asset from outranking a lower-severity issue on a shared identity or recovery service.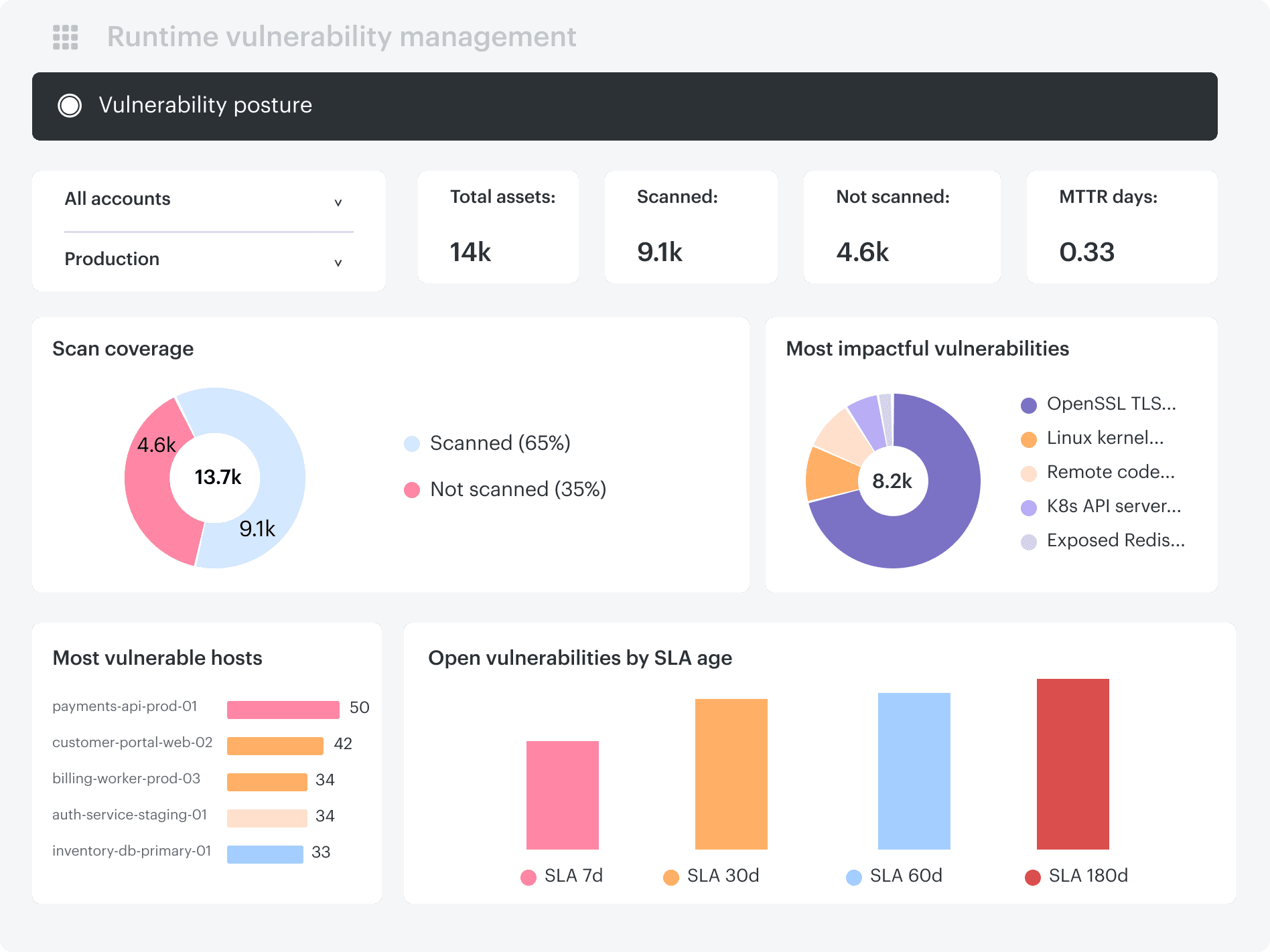 Cloudaware adds asset, ownership, exposure, and remediation context to vulnerability findings across cloud infrastructure.
Cloudaware adds asset, ownership, exposure, and remediation context to vulnerability findings across cloud infrastructure.
See How Cloud Security Posture Management Works for the wider configuration workflow.
5. Track ePHI copies beyond the primary application
A production dataset rarely stays in one place. Analytics jobs, support investigations, disaster recovery, non-production environments, SaaS integrations, and AI workflows all create additional copies outside the original application.
The challenge is that many organizations lose visibility after the first approved transfer.
For example, an analytics export may be copied into object storage, transformed by an ETL pipeline, loaded into a data warehouse, cloned into a test environment, and later retained inside snapshots or backups. Deleting the original record does not necessarily remove every downstream copy.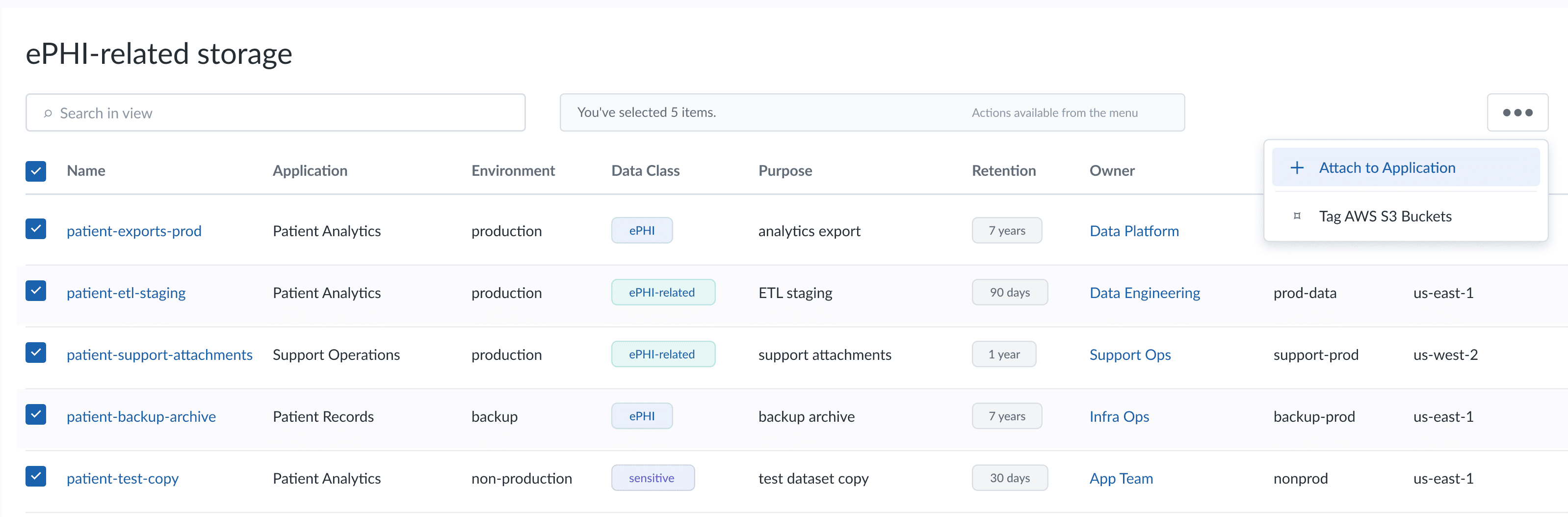 Cloudaware allows teams to extend CMDB objects with custom fields and relationships, making it possible to classify cloud resources by ePHI scope, purpose, requirements, application ownership, or other metadata.
Cloudaware allows teams to extend CMDB objects with custom fields and relationships, making it possible to classify cloud resources by ePHI scope, purpose, requirements, application ownership, or other metadata.
6. Test recovery as a dependency chain
Backup completion does not prove that the healthcare service can be restored. A database may recover while the application remains unavailable because identity, DNS, certificates, encryption keys, queues, network routes, or external integrations are missing.
A recovery test should validate:
- Identity
- Keys and secrets
- Network and DNS
- Data restore
- Application
- Integrations
- Integrity
The proposed HIPAA modernization would require more specific contingency planning and procedures for restoring certain systems and data within 72 hours.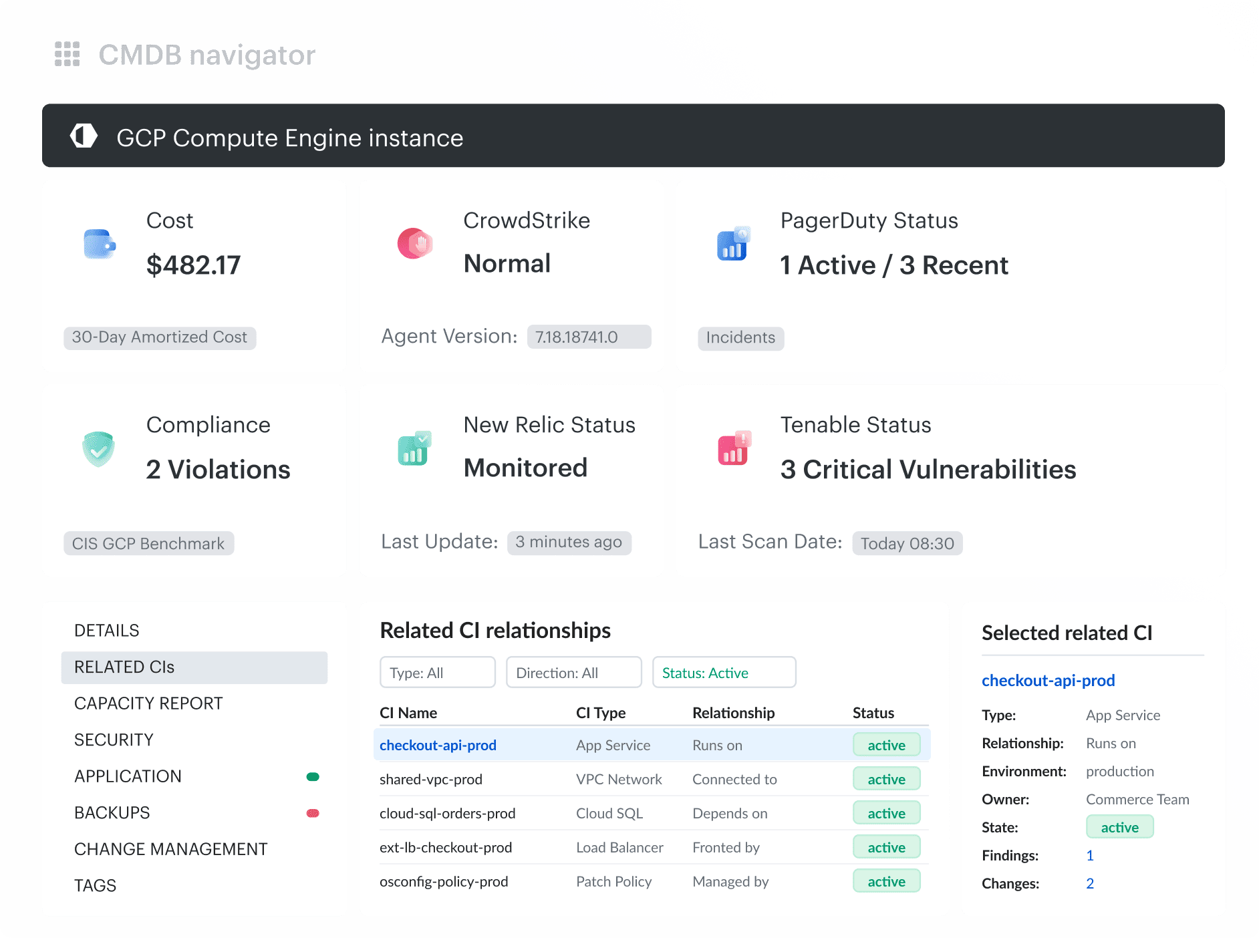 Cloudaware dependency and CMDB context can help identify the assets, owners, and connected services that belong in the recovery test.
Cloudaware dependency and CMDB context can help identify the assets, owners, and connected services that belong in the recovery test.
The broader control lifecycle is covered in Healthcare Data Security.
Healthcare security audit evidence: cloud artifacts auditors expect
Healthcare security audits increasingly test whether risk findings lead to documented action, not whether policies exist. In 2025, HHS OCR announced 21 settlements, many linked to its Risk Analysis Initiative. In April 2026, OCR expanded that initiative to include the HIPAA Security Rule’s risk-management requirements, increasing scrutiny of how identified risks are prioritized, treated, and closed.
Based on audit preparation experience from Katerina L., Cloud Security Expert at Cloudaware, the minimum audit package should let an auditor move from a requirement to a concrete cloud artifact without asking the team to reconstruct the environment.
| Evidence auditors request | Cloud artifact |
|---|---|
| ePHI asset inventory and ownership | CMDB export of in-scope AWS, Azure, and GCP resources with application and owner fields |
| Access control and MFA | IAM credential report, Conditional Access export, privileged-access review |
| Encryption at rest and in transit | Config, Defender, or SCC results; KMS, Key Vault, or CMEK configuration and rotation state |
| Audit-log coverage and retention | CloudTrail, Azure Activity Log, or Cloud Audit Logs configuration showing scope, retention, and destination |
| Vulnerability and patch status | Findings, remediation dates, patch report, and approved exceptions |
| Backup and recovery | Backup configuration and a dated successful restore test |
| Business associate evidence | BAA register, approved-service evidence, and SaaS DPA inventory |
| Incident response | Incident ticket, timeline, breach assessment, and closure record |
| Exceptions | Owner, justification, compensating control, approval, and expiry |
A current configuration export is not enough. Audit evidence must preserve asset identity, timestamp, owner, control state, exception history, remediation, and retest results across the full review period.
How to operationalize continuous healthcare compliance
Continuous healthcare compliance means re-evaluating controls when the environment changes, not simply running scanners more often.
For cloud security engineers, every material change should produce an auditable control event. A new AWS account, internet-facing endpoint, privileged identity, ePHI data flow, or failed restore test should generate:
| Artifact | Required result |
|---|---|
| Scope diff | Assets, identities, and dependencies added or removed |
| Control evaluation | Policy version, query result, and affected CIs |
| Finding | Owner, severity, SLA, and evidence |
| Exception | Compensating control, approver, and expiry |
| Closure | Before-and-after state, ticket, retest, and timestamp |
A finding should reopen when its asset scope changes, an exception expires, or a compensating control fails. Closing the Jira ticket is insufficient; IAM changes require an access recheck, logging failures require an ingestion test, and recovery findings require a successful retest.
Healthcare cloud control evidence with Cloudaware
Cloudaware provides a multi-cloud CMDB and compliance context that can connect resources with owners, findings, vulnerabilities, and operational workflows across AWS, Azure, GCP, VMware, and SaaS environments.
- CMDB: Maintain a live ePHI asset register across AWS, Azure, GCP, Kubernetes, VMware, and SaaS. Add owner, environment, data tier, BAA reference, subcontractor context, and linked findings to each asset record.
- CSPM: Detect misconfigurations that weaken control evidence, including public storage, missing logging, weak IAM, unencrypted assets, expired exceptions, and risky network exposure.
- IT Compliance: Automate evidence collection and control assessment for HIPAA, HITRUST, SOC 2, GDPR, NIST SP 800-66, and internal policies. Reuse one control result across multiple frameworks instead of rebuilding the same evidence package for each audit.
- SIEM: Discover cloud log sources and enrich events with CMDB context. Show which asset, owner, service, and environment produced the event so HIPAA §164.312(b) audit controls can be tied to concrete infrastructure.
- Integrations: Route failed checks into Jira, ServiceNow, PagerDuty, Slack, or the team’s existing workflow. Assign findings to owners, track remediation, and retain closure evidence instead of creating another static export.