






Healthcare data security protects Protected Health Information (PHI) and electronic Protected Health Information (ePHI) after it leaves the Electronic Health Record (EHR) and starts moving through cloud systems, SaaS workflows, operational records, and vendor access paths.
The HIPAA Security Rule defines the safeguard baseline. HHS says the rule establishes national standards for ePHI and requires covered entities and business associates to apply administrative, physical, and technical safeguards.
But the failure usually sits one layer lower: a patient export lands in storage without a data owner, an old service account still reaches a production database, a suppressed finding stays active after the risk changes, and audit evidence no longer matches runtime state.
This guide covers data security in healthcare from the operating layer:
- Where protected health data lives
- Which threats create real risk
- How HIPAA, NIST, and HITRUST map to controls
- How healthcare organizations map PHI exposure to controls and evidence across multi-cloud
Visit our guide to learn about healthcare data security challenges and the 4 biggest threats facing hospitals.
Key insights
- Healthcare data protection starts with scope. Teams need to know which assets create, receive, maintain, or transmit ePHI before they can prove the right controls apply.
- The HIPAA Security Rule gives the baseline, but it does not assign owners, verify cloud implementation, expire exceptions, or keep evidence current across mixed environments.
- PHI exposure is a path problem. An EHR export can land in object storage, feed analytics, appear in logs, get backed up, attach to a support case, and move through a vendor workflow before anyone treats the copy as regulated data.
- Cloud-native tools show provider-specific state. Security teams still need cross-cloud asset context to match findings to owners, policies, remediation work, and audit evidence.
- Healthcare cybersecurity affects care continuity, not only privacy. The American Hospital Association frames cyber risk as a patient-safety issue because disruptions can affect clinical operations and outcomes.
- Breach cost reinforces the operating risk. IBM’s 2025 Cost of a Data Breach Report lists healthcare as the highest-cost industry, with an average breach cost of USD 7.42 million.
What is healthcare data security?
Healthcare data security is the process that protects PHI and ePHI after it leaves the clinical system of record.
In cloud environments, that work starts with 4 questions:
- Where does regulated data exist?
- What can reach it?
- Which control applies?
- What evidence proves the control still matches the environment?
Definition of data security in healthcare
Data security in healthcare protects ePHI from unauthorized access, alteration, loss, and exposure. HHS defines the HIPAA Security Rule as the national standard for ePHI handled by covered entities and business associates.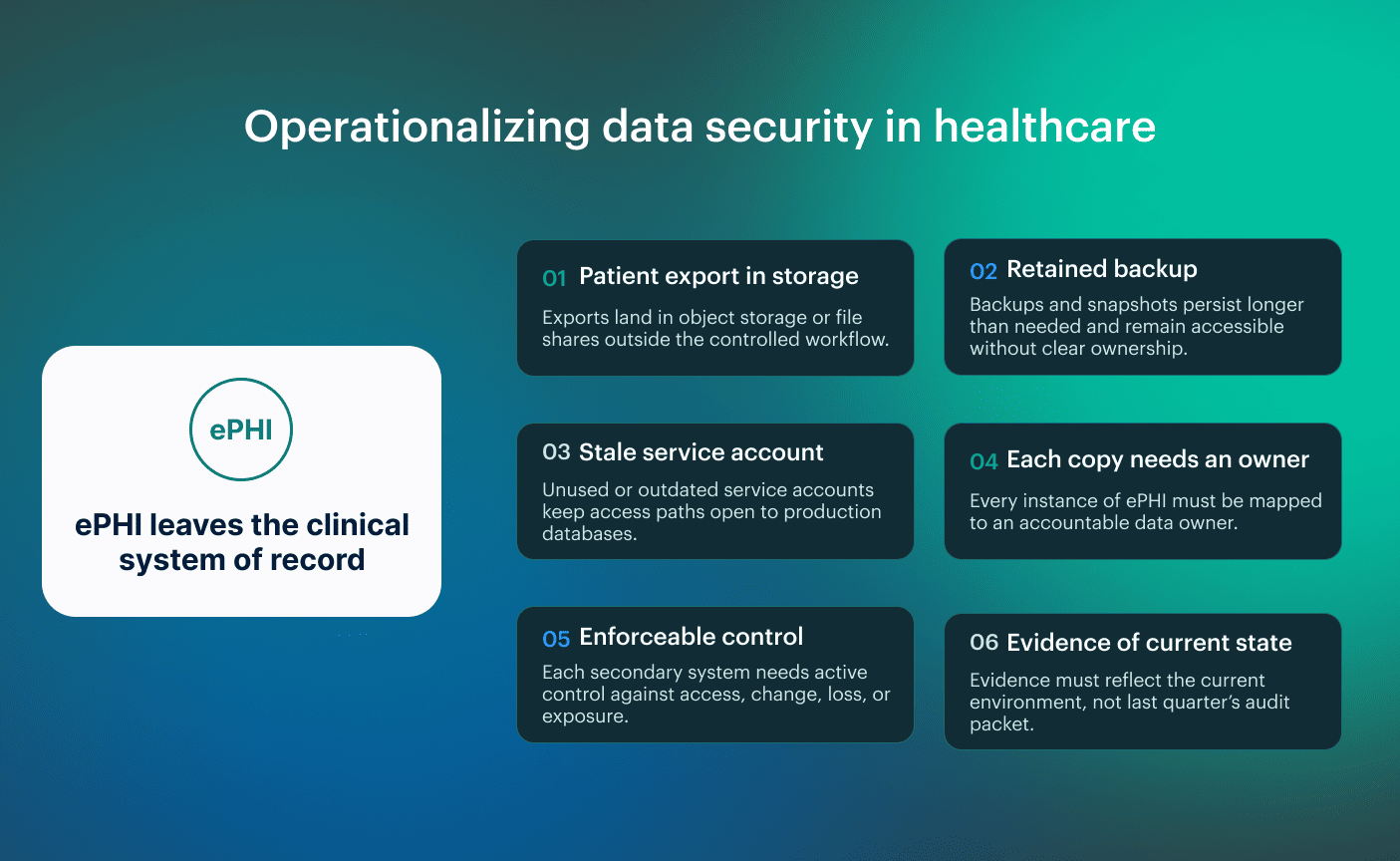 For cloud teams, the definition becomes operational when ePHI moves into secondary systems.
For cloud teams, the definition becomes operational when ePHI moves into secondary systems.
A patient export in storage, a retained backup, or a stale service account with database access can sit outside the workflow everyone assumes is controlled. Each copy needs an owner, an enforceable control, and evidence that reflects the current state, not last quarter’s audit packet.
Data privacy and security in healthcare are related, but not the same
HHS describes the HIPAA Privacy Rule as the national standard for protecting medical records and other individually identifiable health information, while the Security Rule sets administrative, physical, and technical safeguards for electronic PHI.
| Area | Healthcare data privacy | Healthcare data security |
|---|---|---|
| Core question | Is this use or disclosure of PHI allowed? | Is the PHI or ePHI protected against unauthorized access, alteration, loss, or exposure? |
| Primary scope | Privacy: Allowed PHI use and disclosure Security: Safeguards for ePHI systems | Administrative, physical, and technical safeguards for ePHI |
| Example failure | Patient data is shared outside the permitted purpose or contract scope | A permitted export lands in unmanaged storage or keeps excessive access |
| Main evidence | Authorization, permitted-use basis, business associate agreement, disclosure record | Access controls, encryption, logging, backup status, monitoring, configuration state |
| Cloud operating question | Where is PHI allowed to move? | Is every copy controlled, owned, monitored, and provable? |
Privacy may allow patient data to move to a business associate, but security still has to verify that the path is controlled and that evidence matches the current environment. If data lands in unmanaged storage or access survives after the contract scope changes, the privacy decision no longer matches the security state.
Read also: What Are Cloud Security Services? Types, Use Cases, and How to Choose
Importance of data security in healthcare
Healthcare records combine clinical, identity, insurance, and billing value. That is why attackers keep coming back. A breach may expose PHI, but the operational failure often starts earlier, when claims, eligibility, prescriptions, records, or recovery evidence stop moving through the expected control path.
Change Healthcare is the clean proof point because it was not a single-hospital outage. Reuters reported that the breach affected about 192.7 million people, disrupted claims processing across the U.S. healthcare system, and became the largest healthcare data breach in U.S. history.
The control lesson is narrower: healthcare teams need to know which workflow failed, which data path was affected, and who owns recovery.
Patient safety depends on reliable systems and trustworthy data
Patient safety depends on clinical data staying reachable, accurate, and controlled when systems are under stress. If records are unavailable, orders cannot be trusted, or access paths remain open after a workflow change, the security issue has already crossed into operations.
Ransomware shows that failure path clearly. The University of Minnesota Rural Health Research Center found that 84% of ransomware attacks on rural hospitals caused operational disruption, delayed or canceled scheduled care in 42%, and ambulance diversion in 33%. Those are care-delivery consequences, not abstract IT metrics.
So if a patient export lands in unmanaged storage, a vendor service account keeps access after the workflow changes, or lab and order data cannot be reached during downtime, the control has already failed, where the business actually depends on it.
Read also: What Is a Cloud Security Policy? Components, Template & Management
Healthcare cybersecurity threats that drive data risk
Healthcare cybersecurity threats create data risk when they cross a control boundary and gain access to protected health data. The useful unit is the path: credential to system, vendor to workflow, device to service, or exception to unowned finding.
Verizon’s 2025 Data Breach Investigations Report analyzed 22,052 security incidents and 12,195 confirmed breaches, with system intrusion, social engineering, basic web application attacks, and error still driving real breach patterns.
IBM’s 2025 Cost of a Data Breach Report keeps healthcare as the highest-cost industry, with an average breach cost of USD 7.42 million. HHS OCR remains the official breach-reporting record for incidents affecting 500 or more individuals, so the data risk eventually leaves the dashboard and becomes a regulatory event.
The main risk paths are:
- Threat 1: Ransomware and double extortion. Ransomware creates two failures at once: systems become unavailable, and stolen data becomes leverage. In healthcare, that can hit care workflows, payment operations, and breach response in the same incident. The control question is whether recovery paths, identity boundaries, and evidence still hold after systems are isolated or rebuilt.
- Threat 2: Phishing, business email compromise, and stolen credentials. Credential-based attacks matter because healthcare workflows already depend on shared access across providers, payers, support teams, and vendors. A stolen credential does not need to exploit the cloud if it can reach a mailbox, portal, file share, or SaaS workflow that carries PHI.
- Threat 3: Cloud misconfiguration and public storage. Misconfiguration becomes a healthcare data breach path when storage, logs, snapshots, or analytics exports contain PHI and sit outside the intended boundary. Native tools can flag public access or weak logging inside one provider, but the security decision still depends on data sensitivity, ownership, and exception state.
- Threat 4: Over-privileged identities. Stale machine access is where risk survives routine review. Service accounts, workload identities, OAuth apps, and integration users can keep permissions after a workflow changes, which leaves protected health data reachable through paths no one tests until an incident or audit forces the issue.
- Threat 5: Shadow AI and PHI leakage. Shadow AI is a data-loss path with a faster interface. If users paste patient context into an unapproved model, route support notes through an AI workflow, or connect a plugin to patient data without review, the failure is still scope, ownership, and control.
- Threat 6: Medical device and IoMT exposure. Medical devices and IoMT systems add risk when they sit on networks, run legacy software, or depend on vendor-controlled patch cycles. That does not make every device a PHI system, but it does require a mapped path from device or gateway to clinical service, data exposure, and remediation.
Read also: 10 Best Cloud Security Tools in 2026 with Comparison, Pricing, and Honest Reviews
Where protected health data lives in modern healthcare systems
Protected health data does not stay inside the system that everyone calls authoritative. It moves when a hospital sends records to a clearinghouse, syncs a patient portal, runs analytics, opens a vendor case, stores backups, or lets a SaaS workflow process clinical or billing context.
For a hospital data security team, the working question is whether each PHI path still maps to an owned asset, a current control, and evidence that reflects runtime state. HHS uses the “create, receive, maintain, or transmit” scope for ePHI under the Security Rule, which is why secondary systems matter.
PHI can move beyond the EHR into cloud, logs, backups, and SaaS exports
PHI often leaves the EHR through normal work, not an attacker’s first move. Once PHI is maintained or transmitted outside the EHR, that secondary system belongs in the security scope.
Common examples:
- A spreadsheet is shared to complete an operational task.
- A SaaS vendor enables an AI feature that processes patient context.
- A support workflow collects identifiers for troubleshooting.
- A cloud file gets copied into logs, reporting, or backup.
- A business associate keeps access after the original task ends.
So the actual problem is often not malicious behavior, but employees using approved tools faster than security can keep the scope updated. That makes PHI exposure a mapping problem.
| Where PHI moves | Failure mode | Evidence to verify |
|---|---|---|
| Cloud storage | Export kept outside the approved workflow | Storage policy, owner, access log |
| Analytics | Dataset copied or retained beyond need | Classification, access review, retention proof |
| Logs and monitoring | PHI written into broadly accessible logs | Sampling, masking rule, access scope |
| Backups | Backup keeps regulated data after workflow changes | Backup policy, restore test, retention rule |
| SaaS and support | Patient identifiers move into vendor tools | BAA status, owner, deletion proof |
| Service accounts | Stale access survives integration changes | Last-used signal, permission review, ticket trail |
Read also: Multi-Cloud Security Architecture. Reference Model and Best Practices
Healthcare data security standards and regulations
Healthcare data security standards exist to make protection provable. They tell healthcare organizations what must be protected, which controls must exist, and what evidence should survive an audit, breach review, or vendor assessment. The problem starts when each framework becomes its own evidence project.
UpGuard’s healthcare cybersecurity report makes the vendor point directly: if one vendor fails a required condition, third-party compliance becomes a first-party issue.
Key standards and regulations:
- HIPAA Security Rule: Defines safeguards for ePHI. For data security, those safeguards need to map to the real systems that store, process, or transmit regulated data. HHS says the rule requires administrative, physical, and technical safeguards for covered entities and business associates.
- HIPAA Privacy Rule: Defines permitted use and disclosure of PHI. Security teams use it as the approved use case that access and workflow controls need to enforce.
- HIPAA Breach Notification Rule: Defines response duties after unsecured PHI is breached. The practical output is incident scope, affected data, timeline, and defensible evidence.
- HITECH Act: Extends HIPAA accountability and enforcement, including business associate exposure.
- NIST SP 800-66 Rev. 2: Gives practical HIPAA Security Rule implementation guidance for regulated entities. NIST also includes mappings from HIPAA Security Rule standards to NIST Cybersecurity Framework subcategories and SP 800-53 Rev. 5 controls.
- NIST CSF 2.0 / NIST SP 800-53: Helps turn HIPAA requirements into control language security teams can test and audit teams can trace.
- HITRUST CSF: Provides a structured assurance framework for security, privacy, and risk management.
- SOC 2 Type II / ISO 27001 / ISO 27799: Used for vendor assurance, security management, and healthcare information security evidence.
- GDPR Article 9: Applies when health data enters European processing as special category data.
Healthcare data security best practices
Healthcare data security best practices should come from HIPAA Security Rule safeguards, NIST SP 800-66 Rev. 2 implementation guidance, AHA’s patient-safety expectations, and Cloudaware’s field experience with multi-cloud control mapping.
The point is simple: if a PHI path is not tied to an asset, an owner, and evidence, the control is already weaker than it looks.
1. Build PHI-aware asset inventory before enforcing controls
Start by identifying the systems that create, receive, maintain, or transmit ePHI, then tie each one to an owner, environment, and data sensitivity. This comes from HIPAA’s ePHI scope language and NIST’s guidance, which both push teams to know where ePHI exists before they apply safeguards.
That matters because controls do not work well against missing assets. If the asset is not in the security workflow, access checks, encryption status, monitoring, and remediation become partial guesses. Very expensive guessing, usually.
“The fastest way to find weak controls is to compare billing inventory, cloud inventory, and the CMDB. If an asset shows up in one place but not the others, don’t start with severity. Start with ownership.” — Katerina L., Cloud Security Expert at Cloudaware
2. Connect encryption, logging, and recovery to the same asset record
Keep protection and recovery evidence attached to the asset and the environment they protect. HIPAA safeguard logic and AHA state that cybersecurity affects patient safety and care continuity.
A hospital will recover when the team knows which system failed, which data was affected, which backup is usable, and who owns the next action.
Read also: How to Perform a Cloud Security Risk Assessment in 2026
3. Treat access as a data-path control
Access should map to the PHI path it exists to serve, especially service and vendor accounts. This comes from the HIPAA Security Rule’s access-control expectations and from a healthcare SaaS pattern that shows up constantly: approved workflows change, but permissions stay behind.
“In healthcare reviews, I don’t trust access until I can see why it exists. A vendor account that still reaches production after the workflow changed tells you the control model is already out of date.”— Mikhail M., General Manager, Cloudaware
4. Test incident response against real PHI workflows
Run tabletop exercises and response checks against current PHI paths, not generic incident scenarios. This comes from HIPAA breach-response expectations and AHA’s care-continuity framing: exposure often starts with normal work inside approved tools.
A policy can pass review while the real workflow has already changed through file sharing, vendor access, or AI features. Test the workflow people actually use. That is where the failure will show up.
Read also: 9 AWS Cloud Security Best Practices That Pay Off
Vulnerability management for PHI-touching assets
A healthcare organization can have thousands of open vulnerabilities across cloud workloads, containers, internal hosts, and legacy systems. The scanner can rank them by CVSS, but that does not tell the security team which finding can affect PHI, which system is exposed, or which application owner has to act first.
According to the UpGuard report, 73% of healthcare organizations still rely on outdated legacy systems, 85% of IT leaders believe legacy systems threaten their organization’s future, and only 9% of healthcare organizations have prioritized legacy-system removal.
Healthcare providers are protecting PHI-bearing systems, care workflows, and recovery paths, so a finding needs more than a scanner score before it becomes a remediation priority. Build the queue from context:
| Prioritization input | Why it matters |
|---|---|
| CVE and CVSS | Shows what the scanner found and baseline severity |
| KEV status | Shows whether exploitation is already observed |
| Exposure | Separates internet-facing, vendor-reachable, internal, and segmented assets |
| Environment | Separates production, clinical, test, shared, and deprecated infrastructure |
| Data sensitivity | Shows whether the asset touches PHI or supports a PHI workflow |
| Owner and service | Shows who can fix it and what breaks if they do not |
| SLA and exception state | Shows whether the finding is scheduled, overdue, suppressed, or accepted |
In a healthcare vulnerability review, scanner severity alone does not show which assets support regulated-data workflows or lack ownership.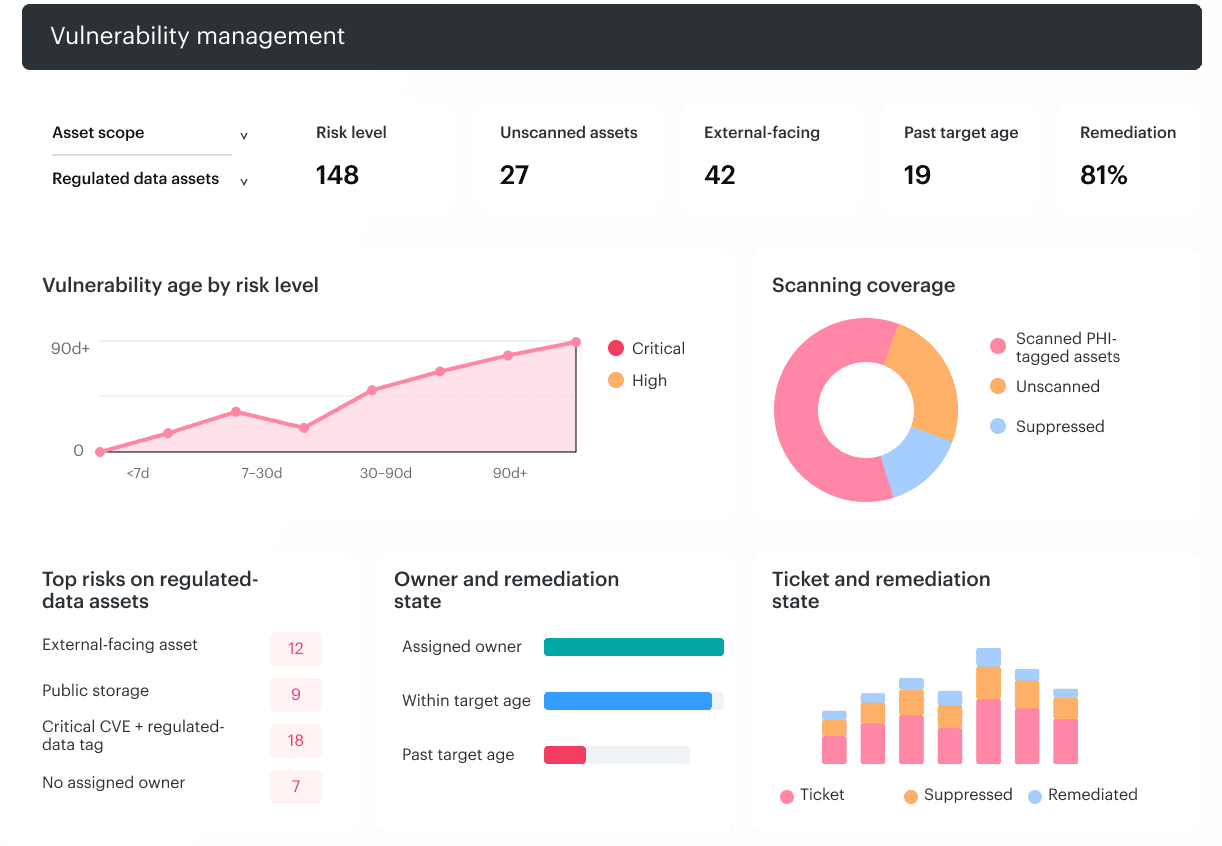 Cloudaware can tie vulnerability data to CMDB records, so teams can review findings with coverage, vulnerability age, unscanned assets, critical-vulnerability aging, and CVE-specific reports instead of working from a disconnected scanner queue.
Cloudaware can tie vulnerability data to CMDB records, so teams can review findings with coverage, vulnerability age, unscanned assets, critical-vulnerability aging, and CVE-specific reports instead of working from a disconnected scanner queue.
Read also: Cloud Security Automation. The Practical Framework for Multi-Cloud Teams
Continuous evidence for HIPAA audits and healthcare compliance
HIPAA compliance in healthcare data security should not live as a separate audit project. Healthcare environments change faster than audit packets, so evidence has to stay attached to active controls.
NIST SP 800-66 Rev. 2 gives regulated entities practical guidance for safeguarding ePHI and understanding the security concepts in the HIPAA Security Rule. For a healthcare security team, the useful interpretation is simple: evidence should come from active controls, not from a manual collection round before audit season.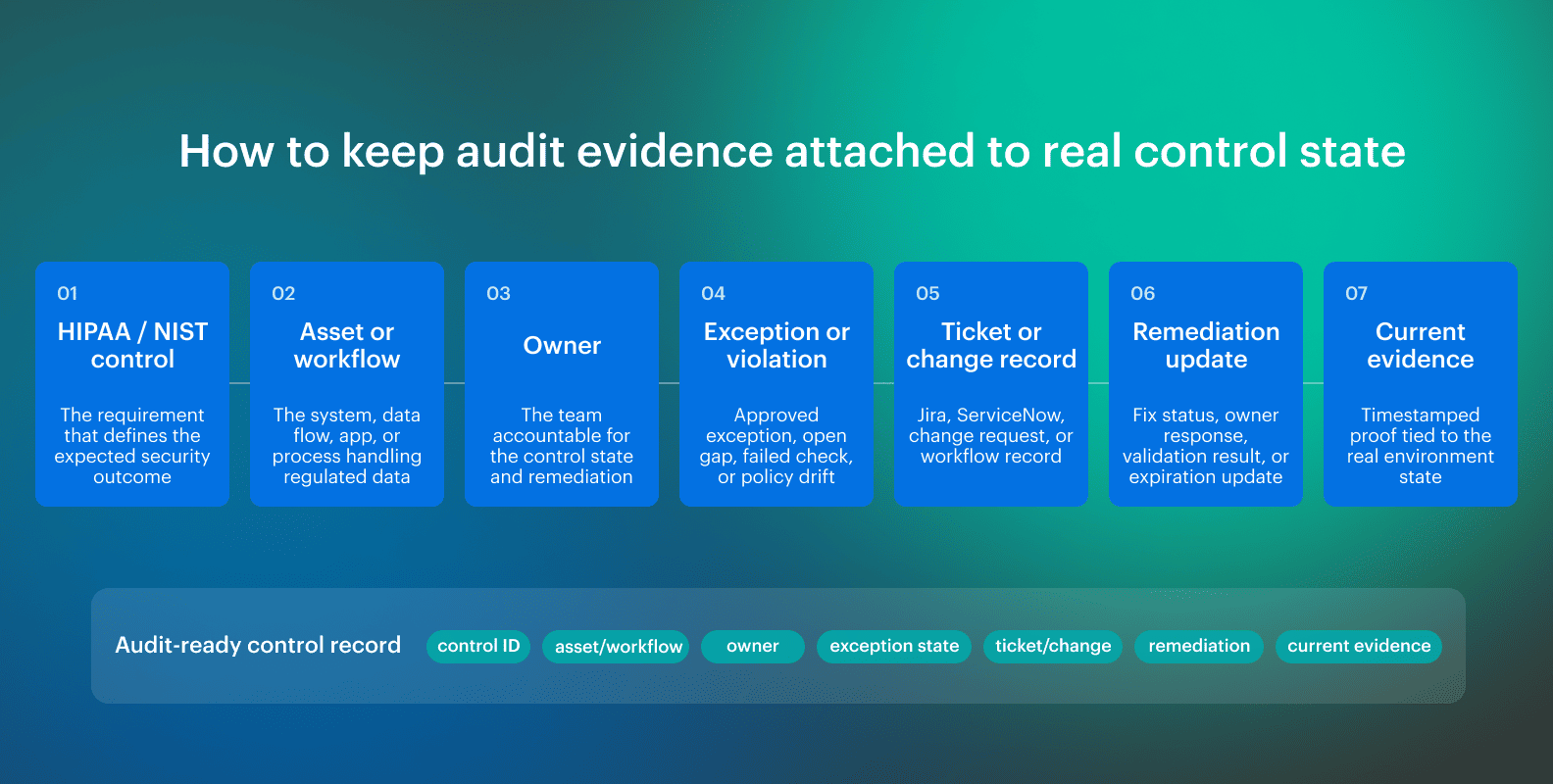 Each evidence item needs to answer six questions:
Each evidence item needs to answer six questions:
- What control does it prove?
- Which asset or workflow does it apply to?
- Who owns it?
- Is there an active exception?
- What record tracks the fix?
- Does the report match the current state?
Read also: Zero Trust Cloud Security. A Practical Multi-Cloud Architecture and Approach
Healthcare data security software: what to look for
A useful healthcare data security platform should do 3 things: keep asset context current, connect findings to owners, and preserve evidence as controls change. If it cannot do that, it is another dashboard.
Look for capabilities that help the team preserve the control path:
- Asset inventory: which cloud, SaaS, virtual, and on-prem systems exist
- Ownership: which team owns the system, service, or workflow
- Posture and compliance: which policy or benchmark the asset violates
- Vulnerability context: which findings matter because of exposure, age, owner, or regulated-data impact
- Exception governance: which risk has been accepted, who approved it, and when it expires
- Workflow: where the finding is routed and how remediation is tracked
- Evidence: what proves the control, ticket, exception, or remediation state is current
Native cloud tools are still required. SIEM, SOAR, IAM, EDR, ticketing, and GRC tools still have jobs. The gap appears between them, where findings lose ownership and evidence gets rebuilt by hand. And if the software cannot preserve that chain across cloud, SaaS, virtual, and on-prem systems, it will definitely not solve healthcare data security.
Read also: 9 Reasons Cloud Security Posture Management Matters in 2026
How Cloudaware supports healthcare data protection in multi-cloud environments
Cloudaware helps healthcare teams move from posture visibility to owned remediation work. Native tools can show that a control failed inside one provider, but the operating problem starts after that: which asset failed, who owns it, whether the exception is valid, and where remediation is tracked. Core capabilities are the ones that keep that chain intact:
Core capabilities are the ones that keep that chain intact:
- CMDB-backed inventory: Track assets across AWS, Azure, GCP, Oracle Cloud, Alibaba Cloud, and on-prem, without depending on one provider console.
- Policy evaluation: Evaluate infrastructure resources against defined policies and create violations when assets fail required conditions.
- Framework-aligned checks: Connect failed checks to frameworks such as PCI, HIPAA, NIST, ISO, GDPR, and CIS Benchmarks for AWS, Azure, and GCP.
- Custom governance: Create custom policies for internal rules such as required tags, approved regions, access patterns, and organization-specific control logic.
- Exception and workflow handling: Manage exceptions, route violations, and escalate issues through Jira, ServiceNow, and ServiceDesk integrations.